Feline Progressive Histiocytosis
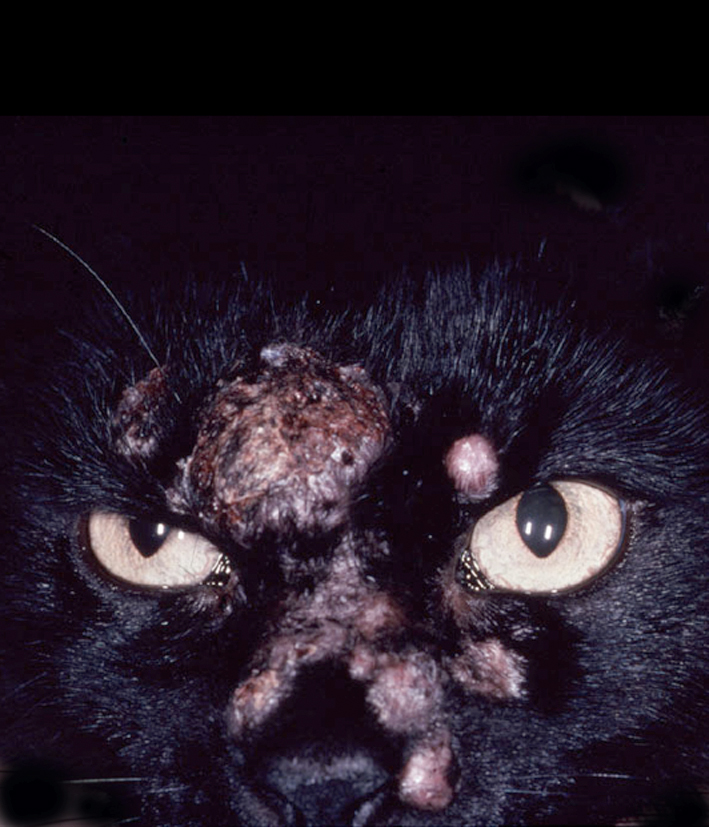
Feline progressive histiocytosis (FPH) is a disease of middle-aged to older cats, the age ranged from 7 to 17 years (Vet Pathol. 2006;43(5):646–655). The initial presentation of FPH many be a solitary skin nodule, although usually multiple papules, nodules or plaques develop, measuring up to 1.5 cm in diameter. The nodules are firm, non-pruritic and non-painful. The surface is often alopecic and may be ulcerated (Fig. 1). The lesions are mostly located on the head, lower extremities or trunk. Occasionally, the lesions are limited to one extremity. The lesions may wax and wane but spontaneous regression does not occur. In FPH, a proportion of cats develop invasive, expansile masses in lymph nodes and internal organs including the lungs, kidneys, spleen, and liver.
Feline progressive histiocytosis behaves as a low-grade HS, which originates in skin from resident interstitial DCs. The initial clinical course is indolent and the histiocytes are cytologically well differentiated, and it is important to rule out infectious agents with special stains. However, later in the course, histiocytes manifest a higher frequency of cytological atypia more consistent with HS (based on serial biopsies from the same cat). Feline progressive histiocytosis has a poor long-term prognosis, since the wide variety of treatments used have lacked efficacy.
Morphologic features
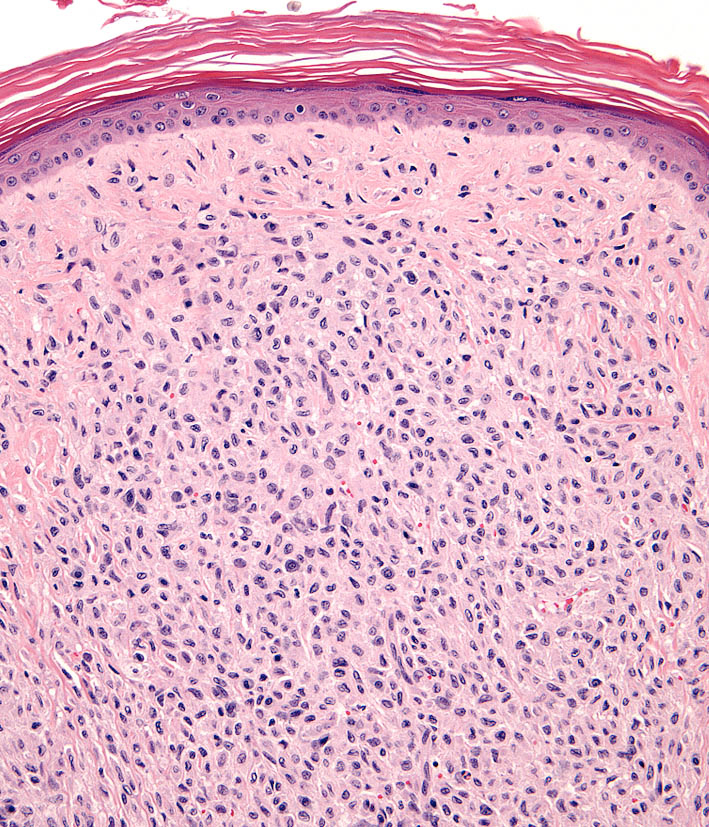
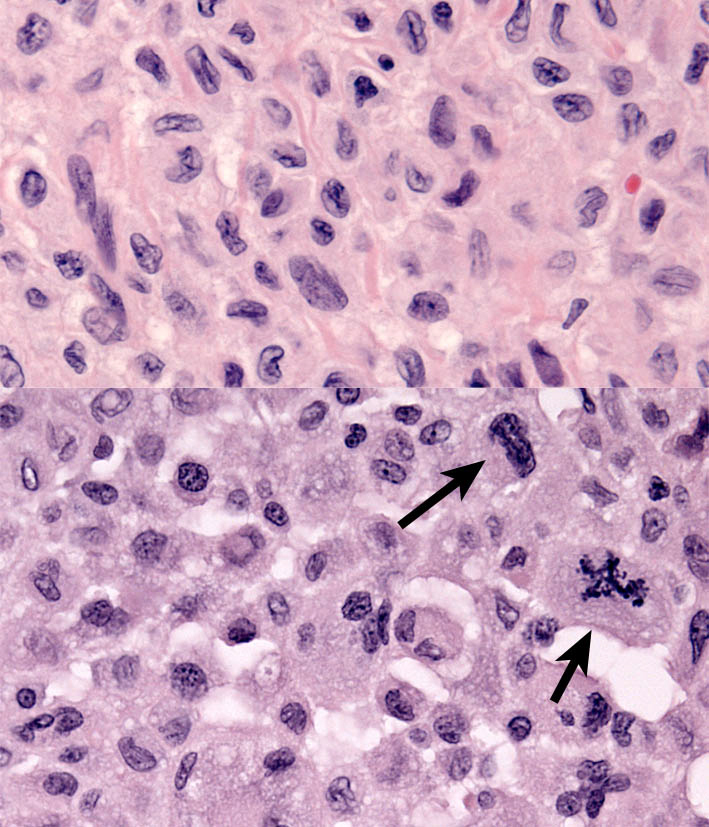
Microscopic lesions consist of diffuse dermal histiocytic infiltrates, which may extend into the subcutis. The overlying epidermis is either intact or ulcerated. Some lesions manifest epitheliotropism (about 40% incidence), characterized by intra-epidermal single cells or cell aggregates, the remaining cases lack epithelial involvement (Fig. 2). Histiocytes have irregular, vesicular nuclei and finely dispersed chromatin (Fig. 3 upper). Electron microscopic investigation of FPH in two cats has not demonstrated BGs (indicative of LC differentiation) in the neoplastic histiocytes. Cytological atypia is present in a minority of lesions early in the course. Biopsies of later lesions (from the same cat) reveal a higher incidence of multinucleated tumor cells. The mitotic activity varies and atypical mitoses are seen (Fig. 3 lower). Late stage lesions are essentially morphologically identical to HS. The extent of reactive infiltrates, composed of dispersed lymphocytes and fewer neutrophils, varies between cases.
Immunophenotypic features
Immunophenotyping of the histiocytes in FPH revealed expression of CD1a, CD18 and MHC class II. The histiocytes most often lacked E-cadherin expression (10% incidence) , and expressed CD5 in about half of the cases. This immunophenotype is most consistent with an interstitial DC origin. The reactive lymphocytes that infiltrate the lesions mostly express CD3 and CD8.
-TOP-